
Valérie Decostre is a physiotherapist and researcher at the Neuromuscular Physiology and Evaluation Laboratory, directed by Jean-Yves Hogrel, at the Neuromuscular Investigation Center of the Institute of Myology. She has just published an article (1) examining the link between strength and muscle function of the hand in Duchenne muscular dystrophy (DMD) and spinal muscular atrophy (SMA). Interview with Valérie Decostre.
What was the background to this study?
The strength and functionality of the hand are fundamental to everyday life. In medical circles, functionality refers to the ability to carry out activities of daily living such as washing, eating, moving around, etc. In neuromuscular diseases, some patients have muscular weakness in their hands, but retain sufficient strength to manipulate an electric wheelchair, a computer mouse or a telephone, for example. Muscular strength not only enables them to carry out hand functions, but also to maintain a degree of independence.
For clinical trials involving neuromuscular diseases such as Duchenne and Becker muscular dystrophies, the European Medicines Agency (EMA) recommends muscle strength and motor function measurements as evaluation criteria.
We wanted to explore the relationship between hand strength and function, which has not yet been described. In particular, at what level of loss of strength in the hand or fingers is there a functional repercussion? Is the progressive loss of muscle strength accompanied by a parallel progressive functional deficit? Does the relationship between hand strength and function differ according to neuromuscular pathologies?
How did you proceed?

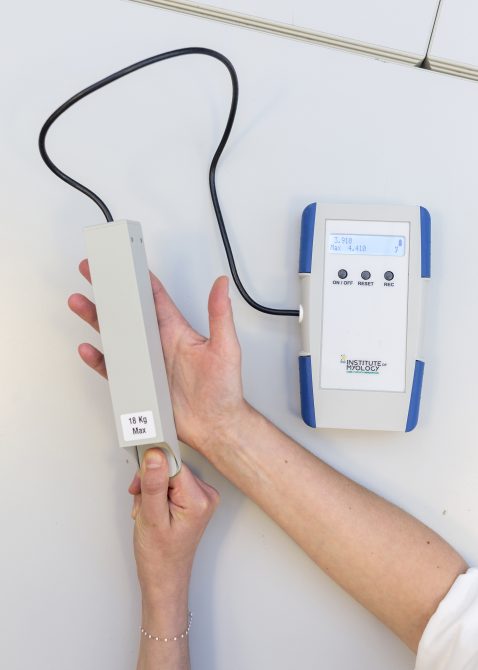
We analysed the strength and function measurements of 168 patients aged between 6 and 31 years, including 91 with DMD and 77 with SMA (60% with type 2 SMA and 40% with type 3 SMA, less severe than type 2) from 3 multicentre observational studies. Hand grip strength was measured using the MyoGrip dynamometer (photo on the left) and the pinch force between the thumb and index finger was assessed using the MyoPinch dynamometer (photo on the right). These devices were designed and developed in our laboratory. They can detect very low forces or very small variations in force.

Hand function was measured in three ways: 1) with the MoviPlate*, a tool that measures coordination and endurance in the fingers, hand and wrist, 2) with the hand-related items of the MFM** scale, where the clinical assessor assigns scores according to the patient’s performance, and finally 3) with the CHFS*** self-questionnaire, where the patient assigns a score according to his or her functional abilities for various manual tasks of daily life.
What did you observe?
Overall, we can see that in DMD and SMA patients (types 2 and 3 combined), hand function is initially preserved despite a progressive loss of grip and pinch strength. Then, when the loss of strength becomes too significant, the function can no longer be ensured and gradually deteriorates. There is therefore a minimum force required for the hand to function optimally. Below this minimum strength requirement, a slight loss of strength can be accompanied by significant functional deterioration. We wanted to determine the minimum force required, below which hand function deteriorates, and whether this minimum threshold force is the same in DMD and SMA.
How did you identify this minimum threshold force?
We used a statistical technique§ to identify the threshold force below which hand function is affected.
When hand function is assessed using the MFM items in patients with DMD, the threshold grip force is 41% of the predicted force§§, i.e. when a patient with DMD has a grip force below 41% of that of a healthy subject of the same age and gender, his or her function will begin to decline. For patients with SMA (types 2 and 3 combined), the grip force threshold is 13% of the force predicted for a healthy subject (% pred). The finger pinch force thresholds were 42% and 26% of the predicted value in DMD and SMA, respectively. The threshold force at which hand function will decline therefore varies according to muscle group (grasp or pinch) and pathology (DMD or SMA).
When hand function is assessed with the Moviplate, the force threshold at which the Moviplate score will deteriorate is 11% of predicted force for patients with DMD and 8% of predicted force for patients with SMA.
For the self-questionnaire, as we did not have enough data to carry out this analysis, we did not identify a threshold force above which the results of the questionnaire show a deterioration in function.
So what did you draw from this?
The relationship between hand strength and function is significant. However, a loss of hand or finger strength only has functional repercussions below a threshold force value that depends on the muscle group and the neuromuscular pathology.
Thus, when patients with DMD develop a maximum grip strength of less than 41% of that of a healthy subject, the function of their hand deteriorates as muscle weakness progresses. In contrast, patients with SMA have preserved hand function as long as their grip strength is not less than 13% of the value predicted for a healthy subject. To explain the difference in threshold force between DMD and SMA, we proposed the following explanation. Patients with DMD often suffer from musculo-tendinous contractures, as do patients with SMA2, but not patients with SMA3. With fewer contractures, SMA patients probably have a wider range of possible motor strategies to compensate for their muscle weakness.
Finally, and most interestingly for me, these results show that normal strength is not essential for a functional hand. And so, if therapies can be used to maintain strength above a certain threshold, we can hope to maintain optimal hand function.
What prospects does this research open up?
For clinicians, it is essential to monitor changes in maximum hand strength in order to prevent, if possible, and anticipate the functional repercussions of a loss of strength.
For clinical trials, knowledge of the relationship between hand strength and function, as well as the strength threshold, should improve the homogenisation of the participants included and the selection of appropriate assessment criteria: (i) If participants whose hand strength is above the threshold and who therefore have little or no functional deficit are included, a therapeutic intervention will only have an impact on strength. (ii) If we include participants whose strength is below the threshold and who therefore present a progressive functional deficit, a therapeutic intervention should have an impact on both the strength and the function of the hand. Thus, while measurement of hand strength will be informative in all cases, functional measures will be relevant primarily in participants with sub-threshold hand strength.
In the future, it would also be interesting to examine the relationship between strength and function in the lower limb, or the upper limb as a whole. We could also try to understand the difference in force thresholds between DMD and SMA: in addition to contractures, which differ in these two diseases, other factors such as dexterity, position perception, skin sensations, bi-manual coordination, arm stability and trunk control contribute to upper limb and hand performance, but remain to be studied in these neuromuscular diseases.
* The MoviPlate has also been designed and developed at the laboratory.
** MFM = Motor Function Measure
*** CHFS = Cochin Hand Function Scale
§ The ROC (Receiver-Operating Characteristic) curve is used in particular to estimate the optimum threshold value for categorising elements (in our case, hand function) into two distinct groups (normal or abnormal function).
§§ The predicted force is calculated using an equation based on the patient’s age and gender. This equation was developed on the basis of force measurements carried out on a large number of healthy subjects. It predicts the average strength that a healthy subject of the same age and gender as the patient in question would develop.
